


Transesophageal Echocardiography
Basics of transesophageal echocardiography for anesthesia in dogs
While historically reserved for cardiac procedures in people, transesophageal echocardiography (TEE) is gaining use as an advanced monitoring tool for noncardiac surgeries. TEE allows the observation of the structure and function of the heart and its valves during anesthesia, in real time, and in a minimally invasive way. “Rescue” TEE protocols provide useful information for assessing sources of hemodynamic instability and valvular competency quickly. Our team has described a rescue TEE protocol for dogs which includes three main views of the heart. Additional views and measurements can be included when there are specific indications. The following clips were acquired from patients in our hospital. We follow the nomenclature described for people.
Note: some of the videos below may take a few seconds to load depending on the speed of your connection.
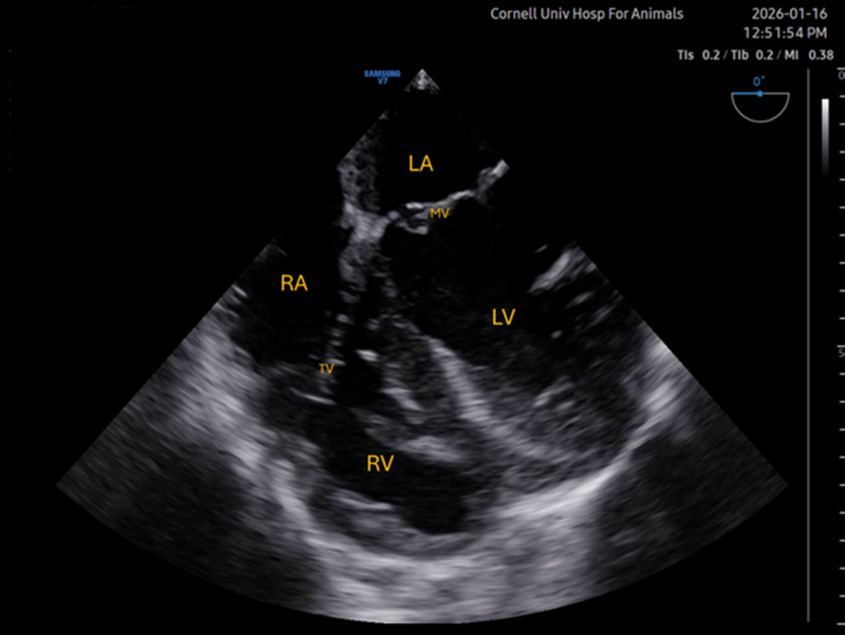
Mid-esophageal four chamber (ME 4C)
This is the first and likely most informative view acquired in most protocols, and often serves as an initial point from which to “move” to other views. Ideally, the image should show the left atrium and ventricle (LA and LV) to the right of the screen, right atrium and ventricle (RA and RV), and atrioventricular valves (MV and TV). Systolic function, volume, and mitral valve competency can be assessed subjectively with this view. This image is typically acquired by situating the tip of the probe over the base of the heart, with the omniplane (multiplanar ultrasound) at 0°. In some dogs, rotation and/or slight anteflexion is often required to optimize the view. Often, the right-sided structures are difficult to visualize.
Photo
Video #1
Video #2
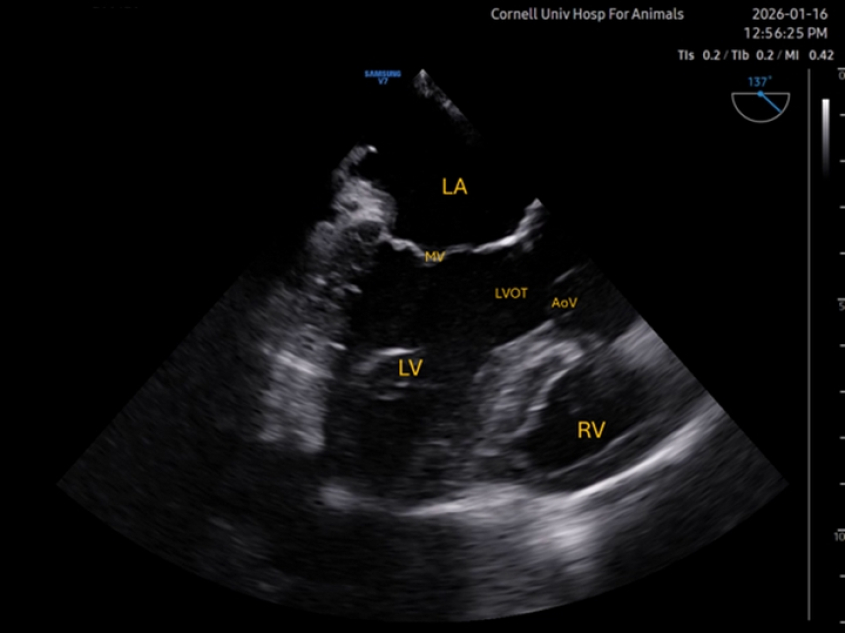
Mid-esophageal long axis (ME LAX)
Rotation of the omniplane to approximately 100° brings the left-ventricular outflow tract (LVOT) and aortic valve (AoV) into view. Color Doppler can be applied over the aortic and mitral valves. The view also allows to assess contractility of different walls than those observed with the ME 4C. In the clip below, insufficiency of both valves can be observed concurrently. In this case, mitral insufficiency was naturally occurring, but the aortic reflux was secondary to placement of a ventricular catheter in our research laboratory.
Picture
Video #1
Video #2
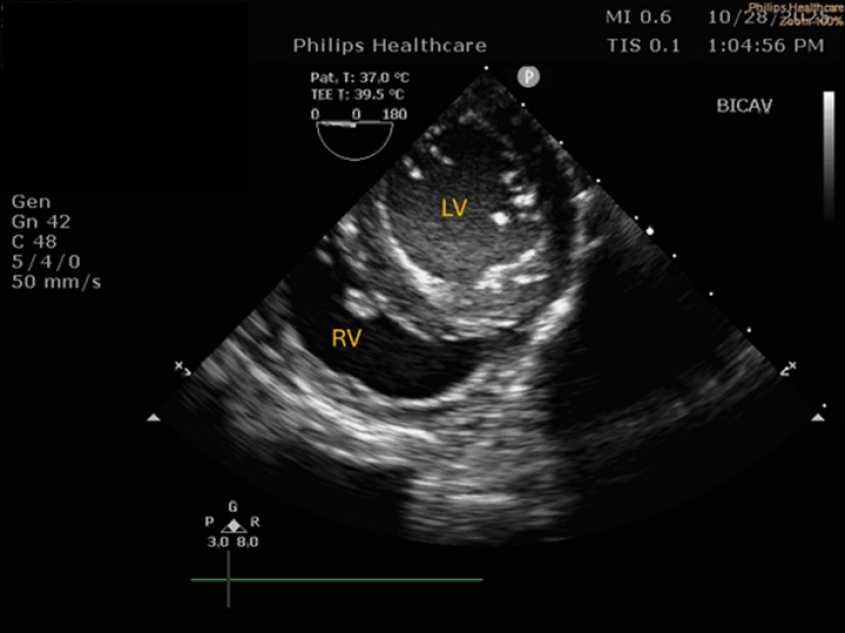
Caudal-esophageal short axis (CE SX)
The short-axis view of the left ventricle – which resembles a mushroom, is typically obtained in people through a deep transgastric location of the probe. This technique is challenging in dogs. An alternative is to obtain this view from a caudal esophageal location, although in our experience, this is not possible in large dogs. Complete, or near complete retroflection of the probe is necessary. The CE SAX view allows to observe all left ventricular walls contract simultaneously, which is useful in humans that may suffer from regional wall motion abnormalities. This problem, however, is much less common in dogs. The view is also useful for volume assessment, and to subjectively judge fractional shortening.
Picture
Video
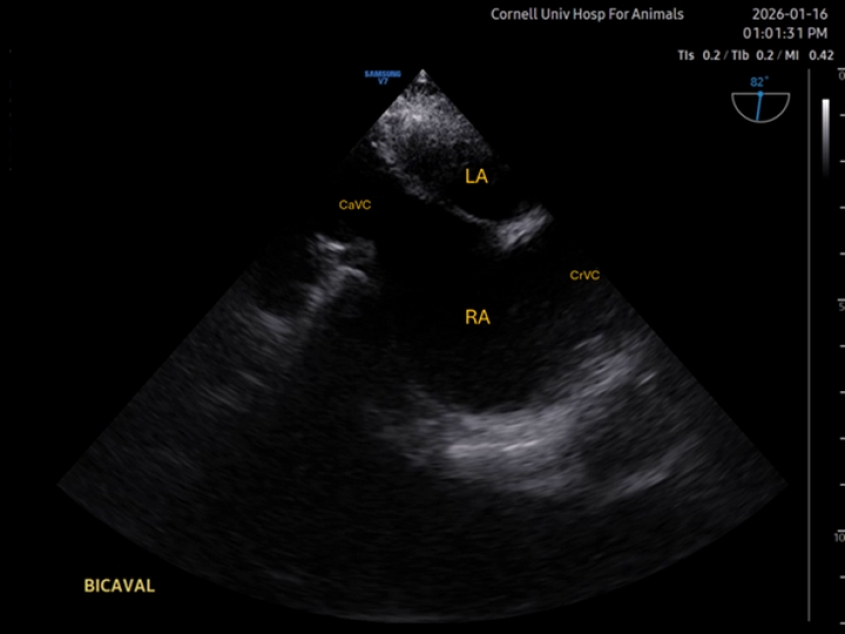
Mid-esophageal Bicaval
The bicaval view shows the left atrium in the near field, and right atrium in the center. The interatrial septum can be observed. Ideally, both cranial and caudal caval veins (CrVC and CaVC) are in view also. The view might be useful for assessing venous return or collapse of the right atrium in cases of tamponade. Additionally, placement of central catheters can be guided with this view. The view is not always easy to acquire. Typically, starting from a ME 4C view centered at the right atrium, or from a short axis of the aortic valve (both with the omniplane at 0°), rotation of the omniplane to 80-110° is applied.
Picture
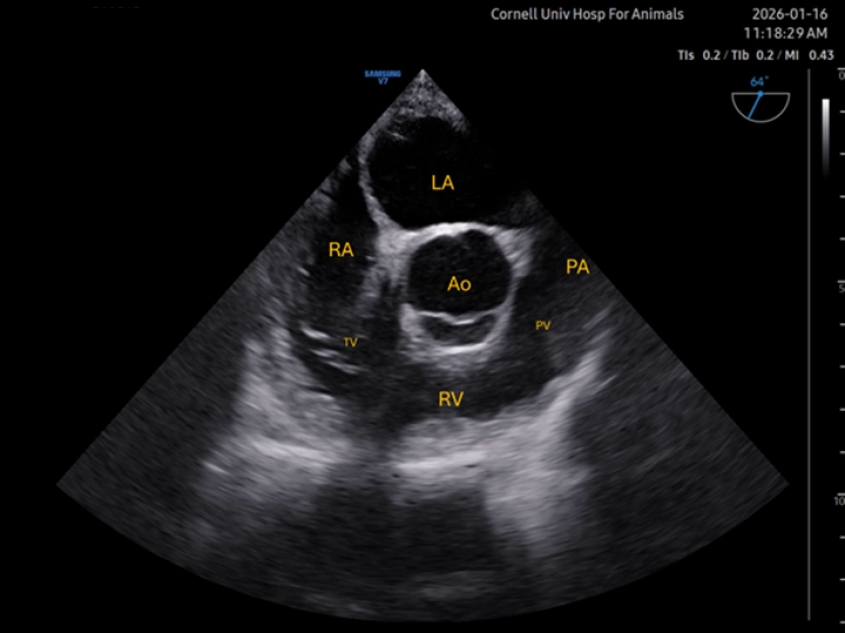
Mid-esophageal right ventricular inflow-outflow (ME RV I-O)
Also starting from a short axis view of the aortic valve, rotation of the omniplane to 60-80° is applied. The probe itself might need to be rotated too in order to bring the tricuspid valve, right ventricle, and pulmonary valve (PV) into view. The pulmonary artery (PA) can be observed too. The aortic valve is typically seen at the center of the image. Reflux through the tricuspid valve can often be assessed on this view, as well as dilation of the right ventricle, often secondary to increases in the afterload. Passage of pulmonary artery catheters can also be guided with this view.
Photo
Video