


Serum Protein Electrophoresis
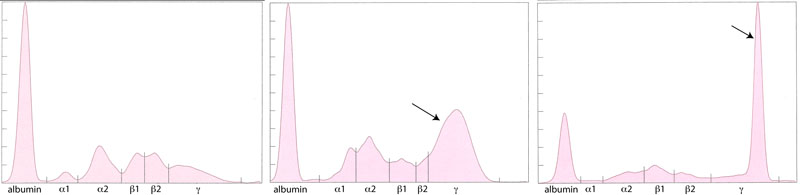
Clinical pathology offers agarose gel serum protein electrophoresis as a test to investigate hyperproteinemia due to hyperglobulinemia. This test can be performed in any species, however we do not have reference intervals for all species. This test can be performed in any species, however we do not have reference intervals for all species. Protein electrophoresis separates serum proteins into different fractions - albumin and α-, β- and γ-globulins - based on their size, shape and charge (Figure 1).
The acute phase proteins migrate in the α-and β- regions of the electrophoretogram and the immunoglobulins comprise the bulk of the γ-region, although IgA, IgM and specific subclasses of IgG can migrate in the late β-region. The shape of the electrophoretogram tracing and the quantity of proteins in β- and γ-fractions, provides information about the underlying disease. In healthy animals, there is a mixture of immunoglobulins, which produces a small broad curve in the γ-region (Figure 1).
Polyclonal versus monoclonal gammopathies
Polyclonal gammopathy
Inflammation, infection or antigenic stimulation of any cause (e.g. chronic liver or dermatologic disease) can induce the secretion of mixed immunoglobulins, resulting in a large broad-based γ- region curve (Figure 2). This is called a polyclonal gammopathy. This pattern is frequently accompanied by a tall, narrow peak in the α-2 globulins, due to increases in acute phase proteins.
Monoclonal gammopathy
Secretion of a single class (and subclass) of immunoglobulins by lymphoid neoplasms will produce a tall narrow peak in the β- to γ-region (Figure 3). This is called a monoclonal gammopathy. A monoclonal gammopathy is usually due to the following:
- Immunoglobulin-secreting B-cell neoplasms, e.g. chronic lymphocytic leukemia or lymphoma
- Plasma cell tumors, e.g. extramedullary plasmacytomas and multiple myeloma.
In these cases, measurement of immunoglobulins can be performed using radial immunodiffusion (RID). Please note, that we can measure IgG, IgM, and IgA with RID in the dog only. We can only measure IgG by this method in cats. B-cell tumors usually produce IgM or IgG monoclonal gammopathies, whereas IgG or IgA monoclonal proteins are typically secreted by plasma cell tumors. Furthermore, the uninvolved immunoglobulins are usually decreased (secondary immunodeficiency) in patients with these neoplasms. Note, that RID testing should never be used alone to identify lymphoid neoplasia. It should always be interpreted with a concurrent electrophoretogram.
|
||
| Figure 1: Electrophoretogram from a healthy dog | Figure 2: Electrophoretogram from a cat with a polyclonal gammopathy due to gingivitis. A broad-based peak is present in the γ-region (arrow) | Figure 3: Electrophoretogram from a cat with an IgG monoclonal gammopathy due to multiple myeloma. A tall narrow peak is present in the γ-region (arrow) |
Unusual gammopathies
“Split monoclonal” gammopathy
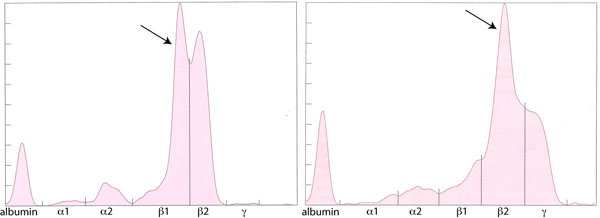
This term is applied when two monoclonal peaks are present (Figure 4). In our experience is usually due to monoclonal IgA (which can dimerize). In rare cases, this can be due to the secretion of two different immunoglobulins, i.e. a true “biclonal” gammopathy. Therefore, RID measurement of the involved immunoglobulin classes is useful in these cases.
“Restricted oligoclonal” gammopathy
This term is applied to a tall narrow “monoclonal-like” peak superimposed upon a broad “polyclonal-like” base (Figure 5). We see this pattern frequently in dogs and cats with immune-mediated, infectious or inflammatory conditions, e.g. severe lymphoplasmacytic stomatitis, Ehrlichia canis infection. It is caused by the stimulation of specific B cells resulting in secretion of a few, restricted classes of immunoglobulins. However, this type of electrophoretogram could also be due to a neoplasm of lymphoid cells in an animal with concurrent antigenic stimulation. Measurement of specific immunoglobulin concentrations is helpful for distinguishing between these possibilities (as is infectious disease testing and diagnostic tests for underlying disease). If the immunoglobulins are mostly IgG, with increased or normal concentrations of IgM or IgA, a “restricted oligoclonal” gammopathy due to infectious, inflammatory or immune-mediated disease is more likely than lymphoid neoplasia.
|
|
|---|---|
| Figure 4: Electrophoretogram from a dog with an IgA-secreting multiple myeloma. Two monoclonal peaks are seen (arrow). Very little protein is observed in the γ-region suggesting concurrent immunodeficiency of the other immunoglobulin classes. | Figure 5: Electrophoretogram from a dog with a restricted oligoclonal gammopathy due to Ehrlichia canis infection. There is a tall narrow peak (arrow) superimposed on a broad polyclonal base in the γ-region. Most of the immunoglobulin was IgG, although IgA and IgM were also increased. |