


Colostrum Collection and Handling, Usage of Refractometer
Colostrum Protocol
"ENOUGH colostrum that is CLEAN and STRONG and fed FAST." ENOUGH colostrum means you need to feed a sufficient volume colostrum to give the calf enough IgG and other immune components; FAST means you need to feed the colostrum within an hour or two of birth; CLEAN means the colostrum cannot be contaminated with potentially infective pathogens; and STRONG means the colostrum must contain a sufficient amount of IgG, immune components and nutrients.
- Collection
- Fresh cows move to milking area within 2 hours of calving
- Milk fresh cows before sick or treated cows
- Cow preparation is identical to routine parlor practices
- Milking equipment is serviced and sanitized between cows and milkings
- Save colostrum for calves only if the cow or heifer meets these criteria:
- Johne's ELISA test negative
- Healthy
- No mastitis
- Has not leaked milk
- No bloody milk
- Has been dry at least 45 days and in the transition group for a minimum of 14days
- Put colostrum into an ice bath immediately after dumping from collection pail. Bacteria start growing soon after harvesting.
- Labeling and Storage
- Fresh colostrum is put into 2 or 4 quart calf bottles or ziplock containers
- Each container is marked with cow ID and date of collection
- Colostrum not fed within 2 hours is placed into a clean refrigerator
- Colostrum > 7 days old is discarded
Target Bacterial Count Guidelines
High bacterial numbers in colostrum can adversely effect the health and well being of dairy calves. Even modest numbers of bacteria (50,000 cfu/ml) can reduce the efficiency of colostrum absorption.
| Sample | Total Bacteria cfu/ml | Total Coliform cfu/ml | Total E. coli cfu/ml |
|---|---|---|---|
| Colostrum | <100,000 | <10,000 | <1,000 |
| Raw Milk | <1,000,000 | Not established | Not established |
| Pasteurized Milk | <20,000 | <1,000 | <100 |
Improving our Handling of Colostrum
Calving Ease May 2010
Summary: The procedures you use to harvest and handle colostrum may determine your rate of treatable scours in young calves. Bacterial contamination of colostrum is common on U.S. and Canadian dairy farms. Controlling this contamination may significantly reduce scours issues among your calves.
Why be concerned about bacteria in colostrum
Field research has shown that even moderate levels of bacterial contamination of colostrum are associated with significant diarrhea problems. This is especially common among calves less than two weeks of age. McGuirk and others demonstrated that farms wanting to avoid scours associated with bacteria in colostrum need to keep levels below these goals (cfu/ml = colony forming units per milliliter):
- Total bacteria less than 100,000 cfu/ml
- Fecal coliforms less than 10,000
- Other gram negatives less than 50,000
- Strep species less than 50,000
- Staph species less than 50,000
- Other less than 5,000
In my dairy consulting work I have found that levels about one-half this high seem to predict scours problems. Regardless of the exact contamination levels, contamination leads to expensive treatment costs and compromised growth in young calves.
How common is bacterial contamination?
Surveys were completed in Pennsylvania and Quebec. In both cases they collected "as-fed" samples of colostrum. When cultured these two-thirds of the samples contained bacteria above the goals listed above. Or, stated the opposite way, only one-third of the colostrum samples had bacteria counts low enough to expect healthy young calves. In Dr. McGuirk’s work in Wisconsin she found that four out of five farms had at least one badly contaminated colostrum sample. I see about this same rate on farms with scours problems.
How to improve collection
- Start with clean teats. Use the "dip-wipe-dip-scrub" prep routine. Collect colostrum into a clean bucket. At the very least the inside of a catch bucket should both look clean and be free of biofilm buildup when checked with your fingers. See www.atticacows.com in Calf Facts for a four-step cleaning protocol.
- Keep the catch bucket covered tightly, both before and after collecting colostrum, any time it is in the milking parlor. Even the smallest amount of cow poop contains huge numbers of coliform bacteria.
How to improve handling
- Feed the fresh colostrum within one-half hour after it is harvested. This prompt feeding gets the colostrum into the calf before bacteria start to multiply. Remember to feed with a clean bottle or tube feeder. All of our efforts to collect clean colostrum can amount to nothing if we inoculate it with our bottle or feeder.
- For colostrum that is to be held for later feeding, chill to at least 60° F (16C) within one half hour. This prompt chilling extends the time for bacteria to double more than seven times (20 minutes at cow body temperature vs. 150 minutes at 60°). An ice-water bath will work well. Or, clean plastic bottles containing ice when dropped into colostrum will work equally well when added at the rate of one quart of ice to one gallon of colostrum.
- When refrigerating the chilled colostrum be sure to store it in clean, sanitized containers. Nursing bottles work fine. Rinse them with a hot strong bleach solution just before filling them. And, put a thermometer in your refrigerator to be sure that the temperature is no higher than 40°F (4C).
- When freezing the chilled colostrum I suggest using the freezer-weight self-sealing plastic bags. I fill the gallon-size bags with just one quart of colostrum. Then, when these are frozen laid flat in the freezer they are thin and thaw quickly.
Relationship between Refractometer Reading and Plasma IgG Level
Plasma IgG Level (mg/mL)
| Refractometer Reading | When fed maternal Colostrum (Quigley) | When fed maternal Colostrum (Tyler) | When fed colostrum Replacer (Quigley) |
|---|---|---|---|
| 7 | 1914 | 2692 | 2225 |
| 6.8 | 1805 | 2512 | 2125 |
| 6.6 | 1696 | 2332 | 2025 |
| 6.4 | 1587 | 2151 | 1924 |
| 6.2 | 1478 | 1971 | 1824 |
| 6.0 | 1369 | 1791 | 1724 |
| 5.8 | 1260 | 1611 | 1624 |
| 5.6 | 1151 | 1431 | 1524 |
| 5.4 | 1042 | 1250 | 1424 |
| 5.2 | 933 | 1070 | 1324 |
| 5.0 | 824 | 890 | 1224 |
| 4.8 | 715 | 710 | 1124 |
| 4.6 | 606 | 530 | 1023 |
| 4.4 | 497 | 349 | 923 |
| 4.2 | 388 | 169 | 823 |
| 4.0 | 279 | N/A | 723 |
Notes:
- Current industry standards suggest 1000 mg/ml IgG as a threshold for passive transfer failure.
- Colostrum replacer manufacturer reports that the ratio between IgG and total protein for maternal colostrum is estimated at 654 while for colostrum replacer it is estimated at 224. This difference is attributed to replacer processing and ingredient selection.
- Equations for IgG values above from Quigley, personal communication. Similar equations for IgG values are in Quigley et al."Absorption of Protein and IgG in Calves Fed a Colostrum Supplement or Replacer." Journal of Dairy Science 85:1243-1248(2002), equations in Figure 2.
- Two sources of maternal colostrum IgG estimates are given to show the variation from study to study of these values. When estimating IgG levels from refractometer readings they are only rough estimates.
Using a refractometer
Measuring the degree of passive transfer in newborn calves can tell you a lot about the level of management in your calf raising enterprise. Studies have consistently shown that the incidence of death and disease is affected by the immunoglobulin (Ig) status of calves shortly after birth. Further, performance of calves (growth, intake, disease resistance) is profoundly affected by their immune status achieved in the first 24 hours. One method used widely to estimate the degree of passive transfer in calves is the refractometer.
This instrument is widely used by veterinarians to determine the overall health status of calves. This Calf Note will provide some insight into the use of a refractometer, and ways to interpret the results.
How does a refractometer work?
The refractometer works by shining a beam of light through a sample of liquid. The device measures the amount of light that is refracted (or bent) from the light path due to the constituents in the sample. In blood, proteins will cause light to bend. The greater the protein, the more light is bent from the light path. In the photo, this student is determining the total protein in a sample of plasma from calves that have just arrived from a sale barn.
What does it measure?
Instead of measuring serum IgG, the refractometer measures total serum protein. In newborn calves, there is usually a close correlation between total protein and IgG in the blood, since largest protein consumed in colostrum is IgG. The correlation between total serum protein and IgG in calves 24 hours of age is approximately 0.71. This means that about 50% of the variation in total protein in the blood of calves at 24 hours of age can be attributed to the IgG fraction (see figure below).
How much total protein is required in my newborn calves?
Most dairy professionals suggest the following guidelines for using total protein to estimate the level of passive transfer in calves?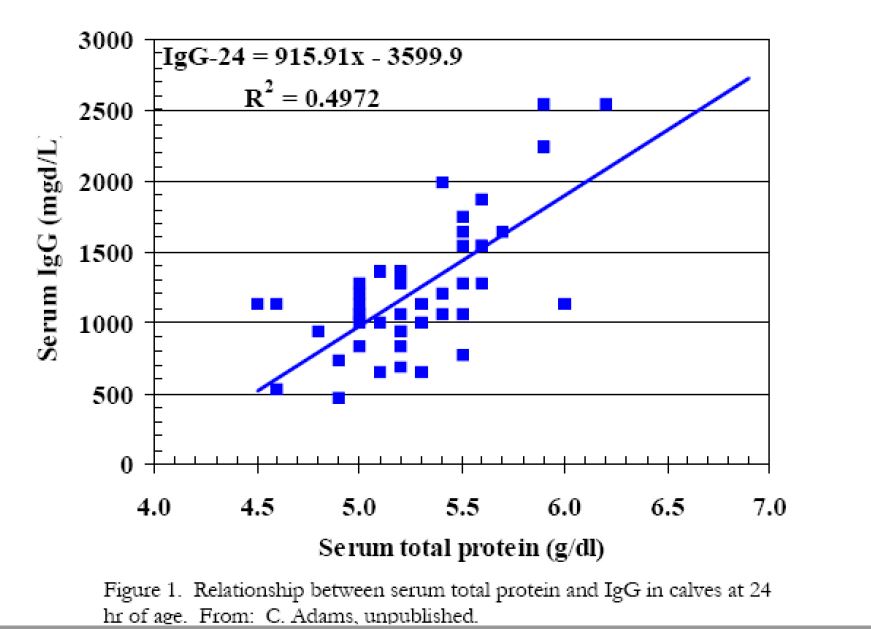
- >5.5 g/dl: successful passive transfer
- 5.0 to 5.4 g/dl: moderately successful passive transfer
- <5.0 g/dl: failure of passive transfer
Note however, in the figure that serum protein of 5.0 g/dl is equivalent to 1,000 mg/dl (or 10 g/L), which many dairy professionals consider successful passive transfer. Using data in the figure, criteria would be:
- > 5 g/dl: successful passive transfer
- 4.75 to 5.0: moderately successful passive transfer
- < 4.75: failure of passive transfer
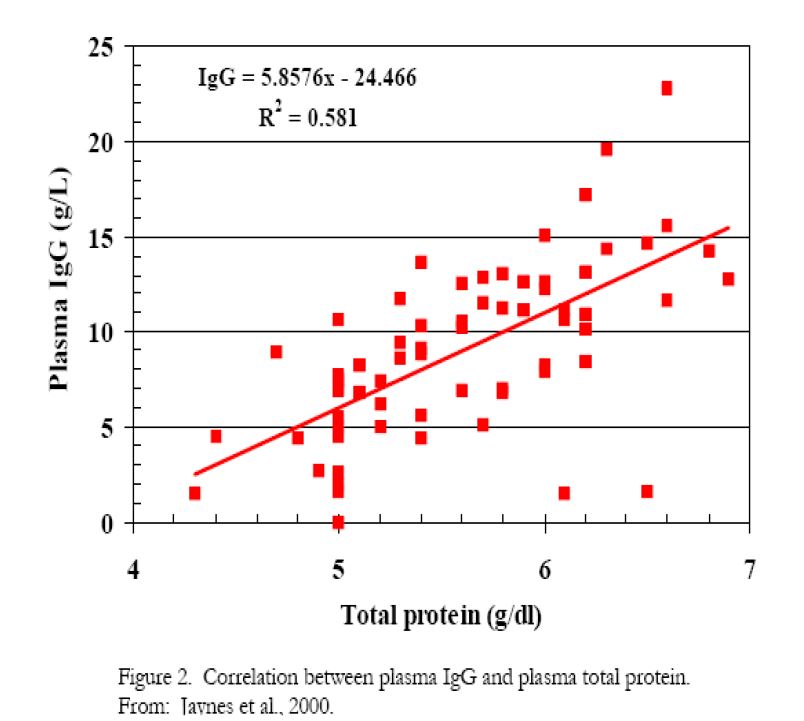
As you can see, the relationship between serum protein and serum IgG is not absolute, and more data is required to identify the reasons for variation among readings and colostral, animal, and environmental factors.
Variation between two different groups of animals is shown in the differences between Figures 1 and 2.
How accurate is it?
 The refractometer is quite accurate in measuring the index of refracted light, which is closely related to total protein in blood. However, there are several factors to consider in determining the validity of the refractometer measurement in estimating the degree of passive transfer in calves.
The refractometer is quite accurate in measuring the index of refracted light, which is closely related to total protein in blood. However, there are several factors to consider in determining the validity of the refractometer measurement in estimating the degree of passive transfer in calves.
The quality of the instrument. Low cost refractometers may be sufficiently accurate to measure the general categories (above), but may not be able to differentiate accurately between small increments of total protein, say between 5.1 and 5.2 g/dl. Check the accuracy and precision of your instrument before purchasing it. The more accurate instruments are generally quite expensive. Generally, on farm refractometers should not be considered experimental instruments. Instead, they should be used as management tools for on-farm application. Highly sophisticated, expensive (>$1,000 U.S.) refractometers may be used in clinical or experimental conditions.
The age of the animal. The relationship between total serum protein and IgG will change as the calf ages. Absorption of dietary proteins other than IgG and movement of IgG from the blood into other body pools can influence the accuracy of the measurement. Therefore, it's best to determine refractometer measurements in calves older than 1 day of age and less than 3 days of age. It's best to wait until the calf is at least 24 hours of age to ensure complete absorption of IgG from the intestine. After about 3 days of age, the relationship between IgG and total protein will change.
The types of proteins absorbed. In normal colostrum, the relationship between IgG and other, non-Ig proteins is fairly constant. Thus, the relationship between refractometer measurements and passive transfer will be satisfactory. However, if the relationship is changed - for example, by using colostrum supplements, then the accuracy of the refractometer may be affected.
What if blood protein is low when measured with a refractometer?
There are several items to consider if your calves don't reach the target level:
The instrument. Be sure the refractometer is working properly. Handle it carefully and take care of it when it is not in use. Regular maintenance, care and calibration will provide you an instrument with a long useful life. Reliance on an instrument that is inaccurate and malfunctioning will only harm the colostrum management program.
The temperature. Refractometers are dependent on the temperature of the sample being measured. Differences in temperature can have a major impact on refractometer readings.
The quality of colostrum fed. If calves are consuming an insufficient mass of IgG, total serum protein (and IgG) will be inadequate. For more information on measuring colostrum quality see Calf Note #22 Using the colostrometer for measuring colostrum quality. Poor quality colostrum is a serious problem for calf growers. Poor quality colostrum may provide inadequate IgG at any realistic colostrum intake. If poor colostrum is a problem, consider using stored colostrum and/or colostrum supplements.
The intake of colostrum. Are calves consuming all the colostrum offered? If not, you should consider using an esophageal feeder to force the calves to consume an adequate volume of colostrum. Of course, intake of large amounts of poor quality colostrum still may not provide adequate serum protein concentration.
The age of the calves. The relationship between total protein and IgG changes as calves get older (see above). Be sure calves are in the appropriate age range for protein measurement when you take blood samples. In addition, the age at which calves are fed colostrum will influence the refractometer measurement. Calves fed colostrum at later ages (> 2-4 hours of age) will not absorb IgG in colostrum as efficiently as calves fed colostrum as soon as possible after birth.
The size of the calves. Larger calves will have a lower serum protein calves compared to smaller calves fed the same mass of IgG. This is because the blood volume of larger calves is greater, and thus, dilutes out the protein (and IgG).
Some of my calves give me extremely high readings - what's going on?
There are a couple of possibilities. First, the calves might be dehydrated. An accurate protein measurement depends on the blood volume. In cases of dehydration, water leaves the circulation, concentrating the other blood constituents. This can lead to very high total protein readings (up to 8 g/dl). Alternatively, check the performance of your refractometer. It may be malfunctioning.
Adding a colostrum supplement to colostrum doesn't make a big difference in calves total protein readings. Why? Again, there are several possibilities that you can't determine differences when adding a commercial colostrum supplement to colostrum:
The colostrum supplement isn't absorbed. Absorption kinetics of some commercial supplements are relatively poor and don't contribute significantly to total protein in the calf.
There's not enough protein in the supplement. Most colostral supplements contain large amounts of protein (>50%) and therefore should contribute to total protein in the calf.
For example, absorption of a 454 gram dose that contains 60% protein will provide 454 x 0.6 = 272.4 grams. If these 272.4 grams are completely absorbed into the blood of a 40 kg calf (assuming 9% plasma volume), then there should be an increase of 75 grams/liter, or 7.5 grams/100 ml. Thus, if a calf has a birth total protein content of 4.0 g/dl, at 24 hours, there should be 11.5 g/dl. This protein concentration is much higher than levels seen in calves, so the total amount of protein in supplements should not contribute to the lack of refractometer increase. Proteins that do not contribute to immune response are typically used for protein synthesis, converted to energy, or are excreted in the urine.
A typical condition, hyperproteinurea, occurs in calves for the first day or so as calves excrete excess protein from colostrum or colostrum supplements.
Calves are fed colostrum and supplement too late. As calves get older, their ability to absorb IgG intact diminishes until the gut "closes" at about 24 hours of age. Feeding colostrum or supplement late (after 12 hours) won't contribute markedly to overall circulating IgG.
The refractometer is not accurate enough to determine differences. Most hand-held refractometers are only accurate to + or - 0.2 g/dl. This means that it cannot effectively distinguish between 5.0 and 5.2 g/dl. Consider the following example. A producer feeds a colostrum supplement in addition to normal, fair quality colostrum (30 g of IgG/L). The producer adds a colostrum supplement that provides 45 grams of IgG. Assuming a typical efficiency of IgG absorption (25%) for both colostrum and supplement, the following will occur:
- initial total protein content of the blood = 4.0 g/dl
- BW of the calf = 40 kg x 0.09 plasma volume = 3.6 L of plasma
- added protein from colostral IgG = 30 g/L x 4 L x 0.25 / 3.6 L of plasma = 0.83 g/dl increase
- added protein from supplement = 45 grams x 0.25 / 3.6 = 0.31 g/dl increase
thus, calves fed colostrum will have 4.0 + 0.8 = 4.8 g/dl; calves fed colostrum + supplement = 4.0 + 0.8 +0.3 = 5.1 g/dl. Depending on the quality of the refractometer, variation in calf body weight, age at first feeding and many other factors, the difference (0.3 g/dl) may not be discernible using a hand-held refractometer. A more accurate clinical refractometer or other tests to directly measure IgG should be used in this case.
Summary
Well, there you have it. The refractometer is a useful tool in managing the colostrum feeding program.Proper use and interpretation of the results can help you in better rearing healthy, productive calves.
Colostrum Supplements and Replacements
Reasons for Use
Failure of passive transfer (FPT) in dairy calves is defined as a blood IgG level of less than 10 mg/mL at 24 to 48 hours after birth. Calves that experience FPT are more likely to become sick or die in the first two months of life than calves with adequate immunity. Many factors can contribute to FPT, but colostrum and the management of colostrum feeding are often involved. All calves should receive colostrum within 2 to 4 hours of birth. Research suggests that calves should be fed at least 100 g of IgG, and feeding 150 to 200 g is recommended to ensure plenty of IgG is available to the calf. Feeding colostrum late or not at all and feeding poor quality colostrum are primary causes of FPT in calves. Unfortunately, not all colostrum is the same.
There is a lot of variability between cows, and all colostrum should be tested to ensure its quality. When available colostrum is low in quality, producers have several options using stored colostrum and products formulated to supplement or replace colostrum. Storing excess high quality colostrum provides insurance in case the dam is unable to produce an adequate quantity of good quality colostrum due to mastitis, death, or various other causes. Stored colostrum from test-negative cows also is an essential component of eradication strategies for diseases such as Johne’s and leukosis. In some herds the supply of disease-free, high quality colostrum is very limited, and supplement and replacer products can provide viable options for ensuring adequate immunity in calves. In other cases, the consistency and convenience of colostrum products is preferred over testing, sorting, and storing maternal colostrum.
Supplement or Replacer - What's the Difference?
Colostrum products that contain IgG are regulated by the USDA Center for Veterinary Biologics. Supplement products are unable to raise the blood concentration of IgG above the species standard, which is 10 mg/mL for calves. Any product that is able to raise serum IgG concentration above 10 mg/mL may be called a colostrum replacer. Colostrum supplements available today are made from dried bovine colostrum or serum and contain 40 to 60 g of IgG per dose (9 to 13% globulin protein). The fat content of these products ranges from 0.5 to 15%. Colostrum supplements can be used to increase the amount of IgG fed to calves when only low or medium quality colostrum is available. However, supplements cannot replace high quality colostrum. Research has shown that when a supplement is added to low quality colostrum, the IgG is often absorbed poorly and calves often experience FPT (see table below). Poor antibody absorption when adding a supplement to colostrum may be due to the large amount of protein entering the intestine in a short period of time. Competition between IgG molecules and other proteins for absorption sites has been suggested as one reason this occurs. Colostrum replacers developed because supplements were not particularly effective.
Supplement products are less expensive than replacer products, but they are less convenient and do not provide a break in the disease transmission cycle because some colostrum must still be fed. One strategy to reduce the overall cost of using these products is to feed a replacer for the first feeding and a supplement for the second feeding. Numerous products designed to replace colostrum are now on the market. These products are made from bovine colostrum or serum and contain 100 to 150 g of IgG per dose. These products also provide fat, protein, vitamins, and minerals needed by the newborn calf, although the amount varies between products. For example, fat content ranges from 6 to 25%.
Colostrum replacer contains more immunoglobulin than supplement products and provides more antibodies than poor or moderate quality colostrum. In an experiment where calves received the same amount of IgG from either colostrum or a serum-based colostrum replacer (Jones et al., 2004), no differences between the calves were observed in IgG levels, efficiency of IgG absorption, incidence of scours, or growth rate during the fi rst month of life. In other trials the amount of IgG transferred to the calves’ blood has been lower in calves fed replacer products than calves fed maternal colostrum; however, the amount of IgG provided by colostrum and replacer products is often different. A University of Minnesota study (Pithua et al., 2010) followed 497 calves from birth through 54 months of age and found no differences in the risk of death or culling, milk production, or reproductive performance of cows that were fed either maternal colostrum or serum-based colostrum replacer at birth. Another part of this project evaluated the risk DAS 11-180 Colostrum Supplements and Replacer 3 of calves becoming infected with Mycobacterium avium subsp paratuberculosis (Pithua et al., 2009) and found calves fed colostrum replacer at birth were less likely to be infected than those fed colostrum.
All calves were born into herds known to have Johne’s disease present, so these results suggest that colostrum replacer can be effective in breaking the transmission from cow to calf. Multiple trials have reported acceptable levels of serum IgG and total protein in calves fed various replacer products (see table below). However, it is important to select products that are proven to be effective, because not all products that have been tested in public research have provided adequate immunity. Generally speaking, the quality and effectiveness of colostrum replacer products have improved in recent years. The table below summarizes the results of 26 research trials published in peer-reviewed journals with nearly 90 different treatments investigating colostrum supplement and replacer products. The table provides a summary of treatment means, which reduces the variability that may have been observed within an individual experiment (or that might occur between individual calves on a farm), but provides a good overview of the performance we can expect on average. Because some of these studies were conducted during the development of replacer products, they provided less than 100 g/dose of IgG. If preliminary studies are removed from the summary to provide a better estimate of products currently on the market, replacer products provided an average of 157 g of IgG, with an absorption efficiency of 31%, and serum IgG of 12 mg/mL. Supplement products (fed in addition to colostrum) provided 136 g of IgG with 19% absorption efficiency and resulted in serum IgG of 9 mg/mL.
Be sure to read and follow the manufacturer’s instructions for feeding; some products are mixed with warm water and fed in an extra feeding, others are added to colostrum, and the number of feedings recommended may vary. Some products packaged in bulk also offer the option of selecting the IgG dose by adding different amounts of powder.
Apparent Efficiency of Absorption (AEA)
The absorption efficiency of calves can be calculated on-farm to determine whether the different factors involved in colostrum feeding are working efficiently. These factors can include timing of first feeding, colostrum quality and amount being fed, of colostrum products being used. Knowing whether the calf has successful passive transfer is most important, however knowing apparent efficiency of absorption can help in trouble shooting.
To calculate apparent efficiency of absorption, the IgG concentration in the blood needs to be known (this is also used to determine passive transfer). Once this has been established, the blood IgG concentration (in g/L, which is the same as mg/mL) is multiplied by the plasma volume in liters (which can be estimated at 9.1% of bodyweight in kilograms for a Holstein calf). This result, the total grams of IgG in the blood, is then divided by the total amount of IgG fed, which can be estimated using a colostrometer for colostrum or found on the label of colostrum supplement or replacer products. The result is then multiplied by 100 to express absorption efficiency as a percentage. As an example, a 45 kg calf will have a plasma volume of 4.1 L (45 kg × 0.091).
Let’s assume the blood IgG concentration tested at 24 hours of age was 8 mg/mL (or g/L) and the calf was fed a total of 100 g of IgG (assuming 2 L of colostrum containing 35 g/L IgG was fed, and due to its poor quality, a supplement was used to provide another 30 g of IgG). Absorption efficiency would be: [(8 g/L IgG × 4.1 L) / 100 g IgG] × 100 = 32.8% AEA This absorption efficiency is very good when we consider that research data suggests maximum absorption efficiencies of around 35% for maternal colostrum. Time of the first colostrum feeding is the most critical factor affecting absorption efficiency, and calf care personnel need to do everything they can to feed colostrum or colostrum products as soon as possible after birth. As mentioned previously, the amount of protein in the calf’s intestine can also influence the absorption of IgG. Providing two smaller feedings of colostrum may be beneficial. Summary of treatment means from 26 published studies investigating colostrum products
Summary
High quality maternal colostrum is still the gold standard for feeding newborn calves. However, colostrum supplement and replacer products can be valuable tools to increase calf immunity when colostrum supplies are limited or disease eradication is desired. Colostrum supplements can be used to increase the amount of IgG fed to calves when no source of quality colostrum is available, but supplements cannot replace high quality colostrum.
They do not contain sufficient quantities of antibodies to raise the blood IgG level in calves beyond what average quality colostrum will do. Colostrum replacer contains greater levels of IgG and other nutrients and provides an effective, convenient method of providing passive immunity to calves when maternal colostrum is not available.
DAS 11-180 Colostrum Supplements and Replacer 6Visit Penn State’s College of Agricultural Sciences on the Web: https://agsci.psu.edu/Penn State College of Agricultural Sciences research, extension, and resident education programs are funded in part by Pennsylvania counties, the Commonwealth of Pennsylvania, and the U.S. Department of Agriculture. Building, University Park, PA 16802-5901, Tel 814-865-4700/V, 814-863-1150/TTY.Originally published in 2005; revised edition published in 2011.
Summary of treatment means from 26 published studies investigating colostrum products
| IgG Intage, g | Number of Means | Average | Maximum | Minimum |
|---|---|---|---|---|
| Maternal Colostrum | 19 | 203 | 447 | 53 |
| Colostrum-based Replacer | 21 | 126 | 210 | 18 |
| Serum-based Replacer | 30 | 129 | 260 | 53 |
| Colostrum-based Supplement | 8 | 157 | 297 | 85 |
| Serum-based Supplement | 4 | 96 | 100 | 90 |
| Serum IgG, mg/mL | Number of Means | Average | Maximum | Minimum |
|---|---|---|---|---|
| Maternal Colostrum | 25 | 16 | 27 | 3 |
| Colostrum-based Replacer | 21 | 11 | 20 | 2 |
| Serum-based Replacer | 30 | 9 | 16 | 5 |
| Colostrum-based Supplement | 8 | 10 | 20 | 5 |
| Serum-based Supplement | 6 | 9 | 11 | 7 |
| Apparent Efficiency of Absorption, % | Number of Means | Average | Maximum | Minimum |
|---|---|---|---|---|
| Maternal Colostrum | 16 | 23 | 36 | 10 |
| Colostrum-based Replacer | 14 | 33 | 51 | 12 |
| Serum-based Replacer | 22 | 25 | 38 | 15 |
| Colostrum-based Supplement | 7 | 12 | 26 | 6 |
| Serum-based Supplement | 4 | 32 | 38 | 25 |
Oxytocin
An excerpt from: A Rational Basis for Therapy in the Sick Postpartum Cow, Grant S. Frazer, BVSc, MS, MBA. Veterinary Clinics Food Animal Practice (2005) 523-568
Oxytocin is the strongest uterotonic agent known [46]. Oxytocin formulations typically contain 20 United States Pharmacopeia (USP) units/ ml, and package inserts recommend dosages of up to 100 USP units (5 mL) [218]. That amount is excessive considering that treatment with as little as 1.0 IU oxytocin will achieve blood concentrations that are comparable with those that occur physiologically during milking. Although a suckling calf will stimulate more oxytocin release than with mechanical milking, the resulting blood levels are still less than those that result from treatment with 10 to 20 USP units oxytocin [219–224]. In other words, an oxytocin dosage of 10 IU is still supra-physiologic. When 50 IU oxytocin was administered IM, the blood levels were increased within 1 minute, and were still above baseline 2 hours later. It appears that absorption of oxytocin from muscle is a slow and continuous process [224]. When oxytocin was given IV at a rate of 0.5 IU/min and at 1.0 IU/min for a period of 60 minutes, there was an initial rapid (T1/23.5–4.0 min) then slower (T1/2 26 min) elimination phase [225].
As little as 2.5 IU of oxytocin IV will cause the proximal ends of the uterine horns to respond within 30 to 50 seconds when progesterone levels are low (2 days before to 2 days after estrus). The increased frequency of myometrial activity persists for up to 80 minutes. If the same dose is administered during estrus itself, the latency period is reduced to 10 seconds, and the frequency of the prolonged rhythmic activity is doubled for about 2 hours [146]. Studies such as this in cycling cows have supported the belief that the myometrium is only responsive to oxytocin when estrogen is dominant. Whether this hormone is effective in cows that have already developed toxic metritis remains to be determined [226,227]. 536 FRAZER
The pain (endorphins) and fear (adrenaline) associated with dystocia manipulations are known to impede uterine motility via an oxytocin block [39,228,229]. In fact, a slow IV infusion of epinephrine (10 mL of 1:1,000) can be used to facilitate manual prolapsing of the postpartum uterus. Relaxation of the uterus is detectable within 1 to 2 minutes of initiating the infusion [15]. The same inhibitory effect on myometrial activity has been demonstrated when adrenaline is administered IV to a cow in estrus [146].Adrenaline exerts a beta-mimetic effect on the estrogen primed uterus (beta2-receptors), thereby suppressing motility [77,230,231]. The pain- and fear-induced uterine atony that is associated with dystocia manipulations can be reversed by the administration of 20 IU oxytocin.
Post-cesareansection fetal membrane retention was reduced from 35% (controls) to 7%(treatment group) when cows received 20 IU oxytocin IM immediately following surgery, and again in 2 to 4 hours [228]. Although some authors suggest that an injection of oxytocin immediately after a routine calvings (not dystocias) may reduce the incidence if fetal membrane retention, there are limited data to support this approach, and the reports are contradictory [192,193,232–237]; however, one report on 175 multiparous cows [238] did indicate that there was a significant reduction in placental retention at 24 hours when cows were treated with 30 IU immediately after calving, and again in 2 to 4 hours. Studies have shown that the mere presence of retained fetal membranes doubles the rate and increases the frequency of uterine contractions [16]. As little as 5 IU of oxytocin IV will initiate a more intense rhythm of contraction in these cows [25]. In two fetal membrane retention studies that reported no beneficial effect of postpartum oxytocin therapy [16,233–235], the authors used what has been demonstrated to be a "spasm-inducing" dose of 60 to 100 IU.
Few studies have attempted to determine what is the most physiologic uterotonic dose of oxytocin [16,19,25].During the first 6 days postpartum, IV doses of oxytocin ranging from 2 USP units up to 40 USP units will increase the frequency of myometrial contractions, with the onset of response occurring approximately 30 seconds after injection. The magnitude of this increase is dependent on both dose and day of treatment [16,25]. Each successively larger dose produces a significantly greater increase in contraction frequency, ranging from 1 every 6.5 minutes (2 USP units) up to 1 every 3 minutes (40 USP units). The last detectable responses to doses of 2, 5, 10, 20, and 40 USP units of oxytocin were observed on postpartum days 6, 7, 8, 9, and 10, respectively. The percentage of uterine body contractions that formed at the end of a propagated tubocervical wave (propagation index) was also increased by all doses of oxytocin. An IV injection of 25 USP units oxytocin at 12 hours postpartum increases the propagation index to 80%dup from the baseline 50% of contractions reaching the uterine body. The same dose of oxytocin (25 USP units) consistently caused an increased contraction frequency (P ! 0.01) and higher tubocervical wave propagation (P ! 0.01) on THERAPY FOR SICK POSTPARTUM COWS 537 treatment days 1 to 5.
The initial response to oxytocin (during the first hour after injection) was similar on days 1 to 5 [16]. On postpartum days 1 to 6, the mean overall duration of response following injection of 20 or 40 USP units of oxytocin (approximately 2 hours and 25 minutes) was significantly greater than that following the lower doses (approximately 1.5 hours). When 25 USP units oxytocin was injected IV, the uterine response lasted at least 2.0 hours on days 1 to 4, but had decreased to 1.5 hours on day 5. Although the overall duration of response was similar following injection of either 20 or 40 USP units, the higher dose caused an initial tetanic like spasm that lasted 6 to 10 minutes.
This tetanic effect was only observed at the 40 USP units dose, and was most marked on the first 3 days postpartum. Three independent studies [16,20,25] have reported that oxytocin’s effect is to not only increase the frequency of uterine contractions, but also the percentage of these contractions that travel completely down the horn to the uterine body. It has been shown that an IV dose of only 5 IU oxytocin resulted in a rapid and strong increase in contractility during the first 2 to 3 days postpartum, but that by days 4 and 5, the amplitude and duration of the response began to decrease [25]. Because the 40 USP units dose causes an initial tetanic spasm, it would appear that most cows are currently being overdosed. The overall duration of response at 2 days postpartum is approximately 3 hours, decreasing and plateauing to 1.5 hours by days 5 to 6 [16]. Thus, the most efficacious oxytocin therapy may need to be adjusted with days postpartum. It has been suggested that a suitable day 2 to 3 protocol may be repeated 20 USP units (1.0 mL) oxytocin injections, administered at least 3 hours apart, or three doses evenly spaced between milkings [187].
By day 4, the dose could be increased to 30 USP units and the frequency increased to every 2 hours. Although this frequent low-dose therapy may be impractical, it certainly would be more physiologic than the widely used, infrequent, tetany-inducing doses [239]. Further studies are required to determine if the long-acting oxytocin formulations could have therapeutic benefit. These products are not currently available in the United States. Because flunixin meglumine attenuates the uterine response to an IV injection of 5 IU oxytocin, doses lower than 20 IU are probably not appropriate when sick cows are being concurrently treated with anti-inflammatory medication [31]. It must be emphasized, however, that in cows that have been treated with flunixin meglumine, uterine involution progresses normally [31].
Pasteurization of Colostrum
Calf Notes.com - Calf Note #96 - Pasteurized colostrum (https://www.calfnotes.com/pdffiles/CN096.pdf)