


Johne’s Disease in Cattle - Article 1
This is the first article in a series presenting current information regarding Johne’s disease in cattle. It is directed toward helping veterinarians and their clients prevent or control this disease and was adapted with permission from the original 1999-2000 series presented by the AABP Food Safety Committee. Content was edited and reviewed by the National Johne’s Working Group and endorsed by the USAHA.
Clinical Description and Epidemiology of Johne’s Disease in Cattle
Prepared and edited by Don Hansen and Christine Rossiter of the AABP Food Safety Committee
Host range
Johne's disease is an infectious bacterial disease that primarily affects the intestinal tract and associated lymph nodes of ruminants. It is a herd problem as well as an individual animal problem because much of the infection is subclinical in nature. Infection, which has varying pathology and signs, is reported in many species of captive, free ranging, and exotic ruminants worldwide; including cattle, sheep, goats, deer, mountain goats, elk, and antelope. Isolated cases are also reported in nonruminants, including horses, rabbits, and nonhuman primates, but these species are not likely significant reservoirs of Johne's disease.
The bacteria that causes Johne's and components of its genetic DNA have been isolated from people with Crohn’s disease (CD), but the significance of this finding is not determined.
The causal agent
Johne’s disease is caused by a mycobacterium called Mycobacterium avium subspecies paratuberculosis (Map). It is a distant relative of the bacteria Mycobacterium bovis, tuberculosis and leprae that cause TB and leprosy in humans and TB in animals. (Map does not cause TB or leprosy.) Map is also very similar to Mycobacterium avium, but is distinguished by presence of an unique IS900 DNA element that is detected by DNA probe.
After ingestion, Map bacteria are taken up by intestinal mucosal cells, especially in Peyer's patches in the ileum, and immediately engulfed by resident macrophages. Map multiplies slowly within the macrophage and if infection is successful it destroys the macrophage and continues to multiply. Map has the clever ability to evade the immune response of the macrophage even after it is turned on. However, not all infections are successful and the immune response in some exposed individuals prevents progression of the initial infection. These mechanisms are largely unknown, but do involve dose and number of exposures, strain and immune biology of the individual. As organisms multiply, they are released and excreted in the feces, which leads to contamination and accumulation in the animal's environment, feed and water.
Infected animals, which multiply and shed bacteria, are the primary source of contamination and exposure to Johne’s disease. The organism does not multiply outside the animal, but the cell wall provides protection that enables it to survive a year or more in most moderate environments. Ultraviolet, heat, and drying, however, can degrade the bacteria.
Signalment of disease
Because of the slowly progressive nature of the infection, cattle may be infected for years before they show any signs of disease.
Once theses signs finally do occur, they include intermittent bouts of diarrhea, which eventually becomes chronic, weight loss and, typically, a good appetite. Some infected animals initially just appear unthrifty. Affected cattle do not generally have a fever. The signs of this disease can easily be confused with several other diseases and may occur with stressful events such as calving, feed changes and relocation. Some data suggests that subclinical stages may result in a decline in performance, especially in milk production, in the last lactation before culling.
Causes of clinical signs
Mycobacteria are taken up by specialized cells (M cells) in the ileum. M cells present the bacteria to macrophages and lymphocytes in Peyer’s patches. The cellular immune system reacts to the invasion by recruiting to the site more macrophages and lymphocytes. Lymphocytes release a variety of cytokines, which enhance the bacterial killing ability of the macrophages.
Macrophages fuse into large cells and with lymphocytes infiltrate infected tissues in large numbers. This leads to the granulomatous thickening of the intestine. In later phases of the immune response, bacteria escape from macrophages into the intestinal lumen and animals begin to shed Map in their feces.
Eventually the bacteria also escape into the vascular system, which stimulates antibody. This humoral immunity, however, does not play a significant role in controlling Map because of its intracellular localization.
Ultimately an ineffective immune response to Map yields a combination of factors that contribute to the development of clinical disease in an individual animal. The factors are poorly understood but involve inflammation and impaired nutrient absorption from the intestine, interaction of systemic and gut immune components, and the eventual collapse of the cellular immune response that allows unhindered proliferation of that infection.
When to suspect a herd is infected
The obvious answer is a herd that exhibits cows with chronic diarrhea and/or weight loss in the face of good appetites. However, some animals may be infected, appear normal, and be culled before any clinical signs are shown. So, some owners may never realize their herd is infected. A common complaint in these herds is that herd production is not as high as it should be.
In attempting to find the cause of low herd production, tests for Johne’s disease on several poor-doing animals is advised. In other herds, owners may see one or more cows with diarrhea or weight loss and suspect Johne’s disease as a possible cause. In chronically infected herds, for each animal with clinical disease, five to 15 other animals may have subclinical infection and not show any signs of Johne’s disease. (See Figure 2.)
Explaining asymptomatic infection
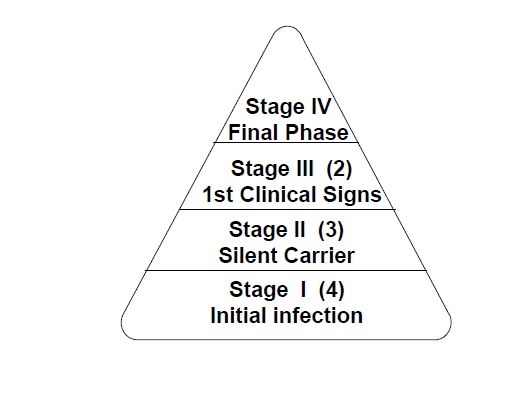
Johne’s is an infectious disease that typically passes through four stages. These stages help explain why infected animals appear healthy for so long and diagnostic tests can’t detect early infection. (See Figure 1.) Stage I is the initial infection: the animal is infected, does not show signs of disease, is not likely to shed bacteria into the environment and is not detectable by diagnostic tests. In Stage II, infection progresses but the animal still does not show any clinical signs. The organism, however, may be excreted in high enough numbers for detection by fecal culture and rarely has antibody detectable by serology. These animals are infectious to other animals. Animals in Stage III show early signs of disease and many diagnostic tests detect infected animals as positive.
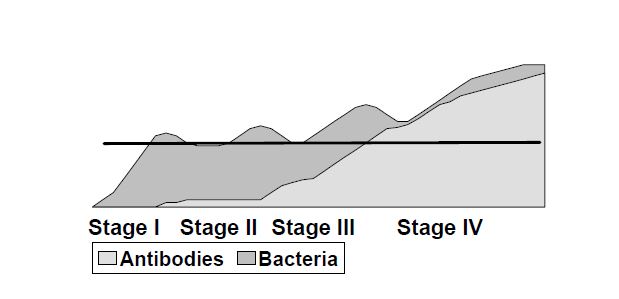
Stage IV is the obvious clinical end-stage of infection. It is readily recognized, terminal, and detected on most diagnostic tests.
In herds with established Johne’s disease, animals are present in all four stages of disease. Depending on the degree of infection and spread, each animal that develops clinical Johne’s disease (Stage IV) may represent five to 15 animals in other stages of infection that don’t show signs.
Common sources of infection
-
The most common source of infection is feces or manure. Except under unusual circumstances, infection begins in the first few months of life. Animals become more resistant with age, though resistance is never complete. If given a sufficiently large dose of the bacteria, adults can become infected.
Nevertheless, under normal animal husbandry conditions, exposure to such large doses probably rarely occurs. This means, for example, that an infected adult dairy cow in a stanchion or tie-stall barn does not infect the cow standing next to her.
Infected cows, however, are the primarily source of infection for calves. In a beef herd, large doses of pathogens may be deposited on ground-fed forages, thus increasing the risk for other animals and especially young stock. Accidentally consuming manure with the bacteria causes the majority of infections in young animals. Suckling manure contaminated teats, licking contaminated bars in the stall where they are born, or being housed in a location with access to manure from the adult herd are ways young animals have opportunities to ingest this microbe. Johne’s disease typically enters a herd when infected, but healthy-looking animals, come in. As the disease progresses in an animal, the frequency and number of bacteria excreted increases. Every day, billions of Johne’s microbes may be excreted from an animal in Stage III or IV of the disease. The infection spreads to calves and herd mates without the owner's knowledge. Eventually signs of the disease may be recognized in one or more animals. - Another source of infection is milk and colostrum from infected dams. The likelihood of Johne’s bacteria being excreted in milk of infected females increases as the disease progresses. Studies suggest that 36% of Stage III and IV cows could have Johne’s microbes in their colostrum and milk. In beef herds, where calves remain with their mothers and nurse daily, the chance for transmission of the infection through colostrum and milk is high. These bacteria may be excreted directly through the mother's milk or may be present in manure of the teats, udder or anywhere calves attempt to suckle.
- In-utero exposure may be a source of infection for calves. It is possible for a fetus to become infected in-utero if the dam is in the later stages of disease. In disease Stages III and IV in the dam, 8% to 40% of fetuses were infected from their mothers in-utero. Infected fetuses can abort or calves can be born that do not display infection until becoming adults. How in-utero infections affect diagnostic tests on those animals that survive to adulthood is not known. Risk for Stage I Stage II Stage III Stage IV Antibodies Bacteria infection of the fetus is low from mothers in disease Stages I and II.
- Water and feed. Water or forages that are contaminated with manure from infected animals are also potential sources of infection. These sources are not well quantified and their risk must be assessed by the degree of contamination, prevalence of infected animals, age and susceptibility of exposed animals. Potential infection sources to consider include shallow, stagnant water sources, forages contaminated during delivery or feeding, poorly drained bogs, over-grazed or heavily manure-contaminated pasture and hay crops sprayed with lagoon waste from infected herds.
Is Map a zoonotic concern?
A debate has developed over the last 15 years about whether Map plays a role in the cause of human Crohn’s Disease (CD). CD is a chronic inflammatory disease of the intestinal tract and therefore bears some resemblance to Johne’s disease in ruminants. CD is most prevalent in the northern, industrialized regions of Europe and North America. Over the last four decades, its incidence trended upward. A quarter to half million people in the US are estimated to suffer from CD. CD typically affects young people, from adolescence to 35 years old.
The cause of CD is not known, but is believed to involve multiple factors, including genetic predisposition plus exposure to some environmental or infectious factor(s). It is generally agreed that CD is the consequence of the intestinal immune system over-responding to some stimulus. Map, other infectious agents, and bacterial or allergic components of the normal intestinal stream are all hypothesized as potential factors to initiate or prolong the immune inflammatory response in CD. Anti-inflammatory drugs, surgical removal of affected intestine, immunomodulating agents, and multi-antibiotic regimens are all used to reduce CD inflammation. There is no cure, however, and individuals with CD continuously alternate between periods of remission and flare-up.
Current evidence is inadequate to determine health risk
Current evidence does not support or reject a causal relationship between Map and CD. Associations do not offer much guidance about the causal relationship between the two factors. CD is a complex disease and extensive research is ultimately needed to determine its cause. The proposed associations with Map are provocative, however, and have helped highlight the need for more research into the cause of CD and have elevated the level of concern by the animal industry that Johne’s may be a food safety issue.
Issues surrounding a possible association between Map and CD include:
Map DNA in CD patients' tissues
DNA detection methods permit researchers to look for the presence of Map in tissue samples by identifying a unique genetic (DNA) component of the bacteria. Several studies in the last decade report finding Map DNA in intestinal tissues taken from CD patients a higher percent of the time than from tissues of control patients with intestinal diseases other than CD. Overall the results conflict since a near equivalent number of studies report different findings, including no Map DNA in CD or non-CD patients, Map similarly present in both groups, and other Mycobacterium also present in each group.
Map bacteria cultured from a few Crohn’s patients
Successful attempts to grow Map from CD patient specimens are rare and the six to eight reported isolations required months to years of incubation. If Map is present in human tissue, proponents of the association suggest that it exists in low numbers and in an adapted form. This form does not grow in the laboratory and lacks a cell wall, which explains why it also cannot be visualized by standard microbiologic methods.
Does milk pasteurization kill Map?
Epidemiologic studies do not offer much evidence for specific factors that may be associated with CD, including milk consumption. However, Map has been cultured from cows with clinical Johne’s disease, thus the role of milk as a possible exposure factor has been considered. In 1996, UK researchers reported that Map DNA was detected in 7% of samples collected in a survey of retail milk samples. Identification of Map DNA does not indicate how much is present or whether the bacterium is living. Subsequently, US and UK researchers conducted experiments on milk samples spiked with Map to determine if current high temperature and short time (HTST, 72C for 15 seconds) milk pasteurization procedures were adequate to kill Map. Different methods had conflicting results. US studies used a turbulent flow lab-scale commercial pasteurizer and reported 100% kill of Map. UK researchers used a holder tube method and showed survival of low numbers of organisms. In 1998, the FDA reviewed the data and stated that commercial HTST pasteurization in the U.S. eliminates the hazard from raw milk products. The batch holder method used by UK researchers is argued to provide less efficient heating than commercial methods.
The UK Food Standards Agency commissioned an investigation by DNA and culture of the Map in 1000 retail milk samples. In efforts to resolve the pasteurization controversy, investigators focused on improving detection of Map by combining techniques to concentrate and grow Map with DNA detection. Full results of the UK study are anticipated in 2001. Preliminary reports indicate that viable Map were recovered from a small percent of raw and retail milk samples. The Food Standards Agency, an independent advisory board in the UK, did not recommend changes in advice on milk consumption or pasteurization procedures, but plans to actively explore all possible controls to reduce the risk of exposure to Map until an association with CD is identified.
A case of Map before Crohn’s
A 1998 published medical case reported the story of a young boy who developed CD five years after being evaluated for enlarged lymph nodes and possible TB. Re-evaluation of the original lymph nodes after CD was diagnosed revealed that the DNA IS900 sequence, which is unique to Map, was present with other Mycobacterium in the lymph nodes. This is the only reported case where Map was demonstrated prior to the development of CD.
Multiple antibiotics may help in Crohn’s
Clinical trials are underway to analyze the effect of treatment with multi-antibiotic regimens on remission of signs and disappearance of CD inflammation. Some patients on long term anti-mycobacterial and broad-spectrum antibiotics had extended periods of remission and reduced symptoms for up to four years after treatment. This is unusual because typical remissions in CD last months to a couple of years. If antibiotic treatments are curative, then a bacterial organism(s) may be at least partially responsible for CD symptoms.
Epidemiologic data do not reveal a cause
Many epidemiological studies were conducted on CD, but none examined specific Map exposure factors, such as direct contact with animals that could have Johne’s disease. The following are examples of some of the more interesting associations that were reported but have not shed much light on possible causes for CD:
- A US study in one state reported a geographic overlap between diagnosed CD. patients and dense dairy cattle areas
- A "hot spot" of CD in the UK exists in a region where water supplies can be contaminated by agriculture-runoff from cattle operations.
- The incidence of CD has a north-south gradient, being highest in northern regions of Europe and North America (highly industrialized countries). Incidence in these regions may now be leveling off but is increasing in southern regions.
- Sweden has one of the highest incidences of CD and one of the lowest of Johne’s disease.
- Family members have a higher risk of CD, which supports a similarity in both genetics and or exposure to some factor.
Note: Information for this article was reviewed by the National Johne’s Working Group, a subcommittee of the Johne’s Committee of the U. S. Animal Health Association. Some of this material was adapted with the kind permission of Michael Collins, Univ. of Wisconsin, at the Johne's Information Center and is also found at the web site http://www.vetmed.wisc.edu/pbs/johnes/.